Physical Therapy And Severs Disease
Overview
Sever's disease involves a lesion to the heel that appears mostly as a result of excessively twisting the ankle. The injury is particularly prevalent in children over 10 and other younger athletes because the heel bone, muscles and tendons are still developing - the bone faster than the muscles - and the condition strikes a growing part of the bone called the calcaneal apophysis. In older people an injury of this sort generally results in a stress fracture.
Causes
Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot.
Symptoms
Pain is usually felt at the back of the heel and around the sides of the heel. If you squeeze the back of the heel from both sides simultaneously and pain is experienced Sever?s disease is more than likely present.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Treatment is primarily directed towards reducing the amount of stress to the heel. Often a heel lift, is placed in the shoe to reduce the pull of the Achilles tendon on the apophysis. Gel or cushioned heel cups may also be helpful in reducing micro trauma to the heel. Orthotic control may also be indicated when a pathologic condition exists in the foot that may be contributing to the increased heel stress. Occasionally, it becomes necessary for adequate healing, to rest the area completely. This can be accomplished either by complete elimination of all strenuous activities, or by using a walking cast or crutches. Often simply reducing activity levels is adequate. Your physician will discuss the best treatment plan with you and your child.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever's disease involves a lesion to the heel that appears mostly as a result of excessively twisting the ankle. The injury is particularly prevalent in children over 10 and other younger athletes because the heel bone, muscles and tendons are still developing - the bone faster than the muscles - and the condition strikes a growing part of the bone called the calcaneal apophysis. In older people an injury of this sort generally results in a stress fracture.
Causes
Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot.
Symptoms
Pain is usually felt at the back of the heel and around the sides of the heel. If you squeeze the back of the heel from both sides simultaneously and pain is experienced Sever?s disease is more than likely present.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Treatment is primarily directed towards reducing the amount of stress to the heel. Often a heel lift, is placed in the shoe to reduce the pull of the Achilles tendon on the apophysis. Gel or cushioned heel cups may also be helpful in reducing micro trauma to the heel. Orthotic control may also be indicated when a pathologic condition exists in the foot that may be contributing to the increased heel stress. Occasionally, it becomes necessary for adequate healing, to rest the area completely. This can be accomplished either by complete elimination of all strenuous activities, or by using a walking cast or crutches. Often simply reducing activity levels is adequate. Your physician will discuss the best treatment plan with you and your child.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Recovering From Posterior Tibial Tendon Dysfunction Surgery
Overview
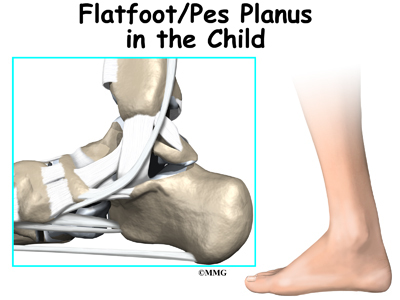
Flatfoot may sound like a characteristic of a certain water animal rather than a human problem. Flatfoot is a condition in which the arch of the foot is fallen and the foot is pointed outward. In contrast to a flatfoot condition that has always been present, this type develops after the skeleton has reached maturity. There are several situations that can result in fallen arches, including fracture, dislocation, tendon laceration, tarsal coalition, and arthritis. One of the most common conditions that can lead to this foot problem is posterior tibial tendon dysfunction. The posterior tibial tendon attaches the calf muscle to the bones on the inside of the foot and is crucial in holding up and supporting the arch. An acute injury or overuse can cause this tendon to become inflamed or even torn, and the arch of the foot will slowly fall over time. 
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility.
Non surgical Treatment
Treatment of Adult Acquired Flatfoot Deformity depends on the stage of progression, as mentioned above paragraphs. Below we will outline a variety of different treatment options available. Orthotics or bracing. To give your foot the arch the support it needs, your podiatrist or foot specialist may provide you with over the counter brace or a custom orthotic device that fits your shoe. Casting. In some cases, a cast or boot is worn to stabilize the foot and to give the tendon time to heal. Physiotherapy. Ultrasound treatments and exercises may help rehab the tendon and muscles. Medications. Over-the-counter (NSAIDS) such as ibuprofen can help reduce pain, inflammation and swelling associated with AAFD. Shoe Gear. Your podiatrist may suggest changes with your shoes you are wearing and inserts you need in your shoe to help support your arch. 
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Adult Aquired FlatFoot
Overview
Acquired flatfoot deformity caused by dysfunction of the posterior tibial tendon is a common clinical problem. Treatment, which depends on the severity of the symptoms and the stage of the disease, includes non-operative options, such as rest, administration of anti-inflammatory medication, and immobilization, as well as operative options, such as tendon transfer, calcaneal osteotomy, and several methods of arthrodesis.
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
At first you may notice pain and swelling along the medial (big toe) side of the foot. This is where the posterior tibialis tendon travels from the back of the leg under the medial ankle bone to the foot. As the condition gets worse, tendon failure occurs and the pain gets worse. Some patients experience pain along the lateral (outside) edge of the foot, too. You may find that your feet hurt at the end of the day or after long periods of standing. Some people with this condition have trouble rising up on their toes. They may be unable to participate fully in sports or other recreational activities.
Diagnosis
The diagnosis of tibialis posterior dysfunction is essentially clinical. However, plain radiographs of the foot and ankle are useful for assessing the degree of deformity and to confirm the presence or absence of degenerative changes in the subtalar and ankle articulations. The radiographs are also useful to exclude other causes of an acquired flatfoot deformity. The most useful radiographs are bilateral anteroposterior and lateral radiographs of the foot and a mortise (true anteroposterior) view of the ankle. All radiographs should be done with the patient standing. In most cases we see no role for magnetic resonance imaging or ultrasonography, as the diagnosis can be made clinically.
Non surgical Treatment
Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Acquired flatfoot deformity caused by dysfunction of the posterior tibial tendon is a common clinical problem. Treatment, which depends on the severity of the symptoms and the stage of the disease, includes non-operative options, such as rest, administration of anti-inflammatory medication, and immobilization, as well as operative options, such as tendon transfer, calcaneal osteotomy, and several methods of arthrodesis.
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
At first you may notice pain and swelling along the medial (big toe) side of the foot. This is where the posterior tibialis tendon travels from the back of the leg under the medial ankle bone to the foot. As the condition gets worse, tendon failure occurs and the pain gets worse. Some patients experience pain along the lateral (outside) edge of the foot, too. You may find that your feet hurt at the end of the day or after long periods of standing. Some people with this condition have trouble rising up on their toes. They may be unable to participate fully in sports or other recreational activities.
Diagnosis
The diagnosis of tibialis posterior dysfunction is essentially clinical. However, plain radiographs of the foot and ankle are useful for assessing the degree of deformity and to confirm the presence or absence of degenerative changes in the subtalar and ankle articulations. The radiographs are also useful to exclude other causes of an acquired flatfoot deformity. The most useful radiographs are bilateral anteroposterior and lateral radiographs of the foot and a mortise (true anteroposterior) view of the ankle. All radiographs should be done with the patient standing. In most cases we see no role for magnetic resonance imaging or ultrasonography, as the diagnosis can be made clinically.
Non surgical Treatment
Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
The Primary Causes And Treatment Plans For Achilles Tendonitis Aches
Overview
 The Achilles tendon connects the calf muscle to the back of the heel. Injuries to the Achilles tendon are common, as it is in constant use during walking and running. These injuries, known as Achilles tendinitis, are usually the result of overuse damage and minor tears that have accumulated over years. Your risk of developing Achilles tendinitis increases with age and activity level. Many athletes develop Achilles tendinitis. The tendon may be injured several inches away from where it attaches to the foot or at the point of attachment. An injury at the point of attachment is called Achilles enthesopathy. We recommend a combination of treatments over a period of months that may include wearing supportive shoes or orthotic devices, performing stretching exercises, and icing the affected area. If these treatments are not effective, or if the tendon is completely torn, we may recommend surgery.
The Achilles tendon connects the calf muscle to the back of the heel. Injuries to the Achilles tendon are common, as it is in constant use during walking and running. These injuries, known as Achilles tendinitis, are usually the result of overuse damage and minor tears that have accumulated over years. Your risk of developing Achilles tendinitis increases with age and activity level. Many athletes develop Achilles tendinitis. The tendon may be injured several inches away from where it attaches to the foot or at the point of attachment. An injury at the point of attachment is called Achilles enthesopathy. We recommend a combination of treatments over a period of months that may include wearing supportive shoes or orthotic devices, performing stretching exercises, and icing the affected area. If these treatments are not effective, or if the tendon is completely torn, we may recommend surgery.
Causes
There are hundreds of tendons scattered throughout our body, but it tends to be a small handful of specific tendons that cause problems. These tendons usually have an area of poor blood supply that leads to tissue damage and poor healing response. This area of a tendon that is prone to injury is called a "watershed zone," an area when the blood supply to the tendon is weakest. In these watershed zones, they body has a hard time delivering oxygen and nutrients necessary for tendon healing, that's why we see common tendon problems in the same parts of the body. Tendonitis is most often an overuse injury. Often people begin a new activity or exercise that causes the tendon to become irritated. Tendon problems are most common in the 40-60 year old age range. Tendons are not as elastic and forgiving as in younger individuals, yet bodies are still exerting with the same force. Occasionally, there is an anatomical cause for tendonitis. If the tendon does not have a smooth path to glide along, it will be more likely to become irritated and inflamed. In these unusual situations, surgical treatment may be necessary to realign the tendon.
Symptoms
The primary symptom of Achilles tendon inflammation is pain in the back of the heel, which initially increases when exercise is begun and often lessens as exercise continues. A complete tear of the Achilles tendon typically occurs with a sudden forceful change in direction when running or playing tennis and is often accompanied by a sensation of having been struck in the back of the ankle and calf with an object such as a baseball bat.
Diagnosis
If you think you have Achilles tendinitis, make an appointment to see your doctor. The doctor will ask you questions about your recent activity and look for signs. The foot not flexing when the calf muscle is pressed ( if Achilles ruptures or tears in half). Swelling on the back of the foot. Pain in the back of the foot. Limited range of motion in ankle. An X-ray or MRI scan can check for tendinitis.
Nonsurgical Treatment
Treatment for achilles tendonitis is based around initially reducing pain and inflammation, stretching the muscles out and a gradual return to activity. No one single approach may cure achilles tendonitis, particularly a chronic condition but a combination of treatment approaches and patience will work best. It is essential the correct treatment is started as soon as possible in the acute stage to avoid the injury becoming chronic. Acute achilles tendonitis requires rest. Continuing to train on a painful achilles tendon could lead to the injury becoming chronic and more difficult to treat. Applying ice or cold therapy as soon as possible to a painful achilles tendon will reduce pain and inflammation. After the first 24 to 48 hours alternating hot and cold or just heat may be more beneficial. Tendons work better when they are warm but if they are painful then rest and ice. Wear a heel pad to raise the heel and shorten the calf muscles which in turn reduces some of the strain on the achilles tendon. This should only be a temporary measure while the achilles tendon is healing. An achilles tendon taping technique can aid rest by supporting the tendon with elastic bandages. This is an excellent way of taking the load off the tendon if you have to walk around on your feet as well as protecting the tendon when returning to full fitness. Achilles tendon exercisesMake sure you have the right running shoes for your foot type and the sport. If you are a runner that over-pronates then a motion control or support running shoe may be needed. Visit a specialist running shop for advice. In the later stages apply heat, especially before exercise. The tendon will perform better when warm. Finish with cold after training to reduce any inflammation.
Surgical Treatment
If non-surgical treatment fails to cure the condition then surgery can be considered. This is more likely to be the case if the pain has been present for six months or more. The nature of the surgery depends if you have insertional, or non-insertional disease. In non-insertional tendonosis the damaged tendon is thinned and cleaned. The damage is then repaired. If there is extensive damage one of the tendons which moves your big toe (the flexor hallucis longus) may be used to reinforce the damaged Achilles tendon. In insertional tendonosis there is often rubbing of the tendon by a prominent part of the heel bone. This bone is removed. In removing the bone the attachment of the tendon to the bone may be weakened. In these cases the attachment of the tendon to the bone may need to be reinforced with sutures and bone anchors.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
The Achilles tendon connects the calf muscle to the back of the heel. Injuries to the Achilles tendon are common, as it is in constant use during walking and running. These injuries, known as Achilles tendinitis, are usually the result of overuse damage and minor tears that have accumulated over years. Your risk of developing Achilles tendinitis increases with age and activity level. Many athletes develop Achilles tendinitis. The tendon may be injured several inches away from where it attaches to the foot or at the point of attachment. An injury at the point of attachment is called Achilles enthesopathy. We recommend a combination of treatments over a period of months that may include wearing supportive shoes or orthotic devices, performing stretching exercises, and icing the affected area. If these treatments are not effective, or if the tendon is completely torn, we may recommend surgery.
Causes
There are hundreds of tendons scattered throughout our body, but it tends to be a small handful of specific tendons that cause problems. These tendons usually have an area of poor blood supply that leads to tissue damage and poor healing response. This area of a tendon that is prone to injury is called a "watershed zone," an area when the blood supply to the tendon is weakest. In these watershed zones, they body has a hard time delivering oxygen and nutrients necessary for tendon healing, that's why we see common tendon problems in the same parts of the body. Tendonitis is most often an overuse injury. Often people begin a new activity or exercise that causes the tendon to become irritated. Tendon problems are most common in the 40-60 year old age range. Tendons are not as elastic and forgiving as in younger individuals, yet bodies are still exerting with the same force. Occasionally, there is an anatomical cause for tendonitis. If the tendon does not have a smooth path to glide along, it will be more likely to become irritated and inflamed. In these unusual situations, surgical treatment may be necessary to realign the tendon.
Symptoms
The primary symptom of Achilles tendon inflammation is pain in the back of the heel, which initially increases when exercise is begun and often lessens as exercise continues. A complete tear of the Achilles tendon typically occurs with a sudden forceful change in direction when running or playing tennis and is often accompanied by a sensation of having been struck in the back of the ankle and calf with an object such as a baseball bat.
Diagnosis
If you think you have Achilles tendinitis, make an appointment to see your doctor. The doctor will ask you questions about your recent activity and look for signs. The foot not flexing when the calf muscle is pressed ( if Achilles ruptures or tears in half). Swelling on the back of the foot. Pain in the back of the foot. Limited range of motion in ankle. An X-ray or MRI scan can check for tendinitis.
Nonsurgical Treatment
Treatment for achilles tendonitis is based around initially reducing pain and inflammation, stretching the muscles out and a gradual return to activity. No one single approach may cure achilles tendonitis, particularly a chronic condition but a combination of treatment approaches and patience will work best. It is essential the correct treatment is started as soon as possible in the acute stage to avoid the injury becoming chronic. Acute achilles tendonitis requires rest. Continuing to train on a painful achilles tendon could lead to the injury becoming chronic and more difficult to treat. Applying ice or cold therapy as soon as possible to a painful achilles tendon will reduce pain and inflammation. After the first 24 to 48 hours alternating hot and cold or just heat may be more beneficial. Tendons work better when they are warm but if they are painful then rest and ice. Wear a heel pad to raise the heel and shorten the calf muscles which in turn reduces some of the strain on the achilles tendon. This should only be a temporary measure while the achilles tendon is healing. An achilles tendon taping technique can aid rest by supporting the tendon with elastic bandages. This is an excellent way of taking the load off the tendon if you have to walk around on your feet as well as protecting the tendon when returning to full fitness. Achilles tendon exercisesMake sure you have the right running shoes for your foot type and the sport. If you are a runner that over-pronates then a motion control or support running shoe may be needed. Visit a specialist running shop for advice. In the later stages apply heat, especially before exercise. The tendon will perform better when warm. Finish with cold after training to reduce any inflammation.
Surgical Treatment
If non-surgical treatment fails to cure the condition then surgery can be considered. This is more likely to be the case if the pain has been present for six months or more. The nature of the surgery depends if you have insertional, or non-insertional disease. In non-insertional tendonosis the damaged tendon is thinned and cleaned. The damage is then repaired. If there is extensive damage one of the tendons which moves your big toe (the flexor hallucis longus) may be used to reinforce the damaged Achilles tendon. In insertional tendonosis there is often rubbing of the tendon by a prominent part of the heel bone. This bone is removed. In removing the bone the attachment of the tendon to the bone may be weakened. In these cases the attachment of the tendon to the bone may need to be reinforced with sutures and bone anchors.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
What Exactly Triggers Pain At The Heel

Overview
Heel pain is a common foot condition. It's usually felt as an intense pain when using the affected heel. Heel pain usually builds up gradually and gets worse over time. The pain is often severe and occurs when you place weight on the heel. In most cases, only one heel is affected, although estimates suggest that around a third of people have pain in both heels. The pain is usually worse first thing in the morning, or when you first take a step after a period of inactivity. Walking usually improves the pain, but it often gets worse again after walking or standing for a long time. Some people may limp or develop an abnormal walking style as they try to avoid placing weight on the affected heel.
Causes
Although plantar fasciitis may result from a variety of factors, such as repeat hill workouts and/or tight calves, many sports specialists claim the most common cause for plantar fasciitis is fallen arches. The theory is that excessive lowering of the arch in flat-footed runners increases tension in the plantar fascia and overloads the attachment of the plantar fascia on the heel bone (i.e., the calcaneus). Over time, the repeated pulling of the plantar fascia associated with excessive arch lowering is thought to lead to chronic pain and inflammation at the plantar fascia’s attachment to the heel. In fact, the increased tension on the heel was believed to be so great that it was thought to eventually result in the formation of a heel spur.
Symptoms
Pain is the main symptom. This can be anywhere on the underside of your heel. However, commonly, one spot is found as the main source of pain. This is often about 4 cm forward from your heel, and may be tender to touch. The pain is often worst when you take your first steps on getting up in the morning, or after long periods of rest where no weight is placed on your foot. Gentle exercise may ease things a little as the day goes by, but a long walk or being on your feet for a long time often makes the pain worse. Resting your foot usually eases the pain. Sudden stretching of the sole of your foot may make the pain worse, for example, walking up stairs or on tiptoes. You may limp because of pain. Some people have plantar fasciitis in both feet at the same time.
Diagnosis
Your doctor may look at your feet and watch the way you stand, walk and exercise. He can also ask you questions about your health history, including illnesses and injuries that you had in your past. The symptoms you have such as the pain location or when does your foot hurts most. Your activity routine such as your job, exercise habits and physical activities preformed. Your doctor may decide to use an X-ray of your foot to detect bones problems. MRI or ultrasound can also be used as further investigation of the foot condition.
Non Surgical Treatment
A steroid (cortisone) injection is sometimes tried if your pain remains bad despite the above 'conservative' measures. It may relieve the pain in some people for several weeks but does not always cure the problem. It is not always successful and may be sore to have done. Steroids work by reducing inflammation. Sometimes two or three injections are tried over a period of weeks if the first is not successful. Steroid injections do carry some risks, including (rarely) tearing (rupture) of the plantar fascia. Extracorporeal shock-wave therapy. In extracorporeal shock-wave therapy, a machine is used to deliver high-energy sound waves through your skin to the painful area on your foot. It is not known exactly how it works, but it is thought that it might stimulate healing of your plantar fascia. One or more sessions of treatment may be needed. This procedure appears to be safe but it is uncertain how well it works. This is mostly because of a lack of large, well-designed clinical trials. You should have a full discussion with your doctor about the potential benefits and risks. In studies, most people who have had extracorporeal shock-wave therapy have little in the way of problems. However, possible problems that can occur include pain during treatment, skin reddening, and swelling of your foot or bruising. Another theoretical problem could include the condition getting worse because of rupture of your plantar fascia or damage to the tissues in your foot. More research into extracorporeal shock-wave therapy for plantar fasciitis is needed. Other treatments. Various studies and trials have been carried out looking at other possible treatments for plantar fasciitis. Such treatments include injection with botulinum toxin and treatment of the plantar fascia with radiotherapy. These treatments may not be widely available. Some people benefit from wearing a special splint overnight to keep their Achilles tendon and plantar fascia slightly stretched. The aim is to prevent the plantar fascia from tightening up overnight. In very difficult cases, sometimes a plaster cast or a removable walking brace is put on the lower leg. This provides rest, protection, cushioning and slight stretching of the plantar fascia and Achilles tendon. However, the evidence for the use of splint treatment of plantar fasciitis is limited.

Surgical Treatment
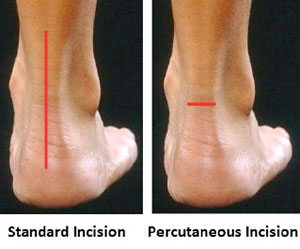
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.
Prevention
Factors that help prevent plantar fasciitis and reduce the risk of recurrence include. Exercises to strengthen the muscles of the lower leg and ankle. Warming up before commencing physical activity. Maintaining a healthy body weight. Avoiding high heeled footwear. Using orthotic devices such as arch supports and heel raises in footwear, particularly for people with very high arches or flat feet. Daily stretches of plantar fascia and Achilles tendon.
What Is Pain In The Heel And The Right Way To Fix It

Overview
Plantar Fasciitis is a common athletic injury of the foot. While runners are most likely to suffer from plantar fasciitis, any athlete whose sport involves intensive use of the feet may be vulnerable. The risk of plantar fasciitis increases in athletes who have a particularly high arch, or uneven leg length, though improper biomechanics of the athlete’s gait and simple overuse tend to be the primary culprits. If you suffer from plantar fasciitis or are seeking to prevent its occurrence it is important to follow the information in this article. In addition, adding a few simple stretches to your fitness program will also help.
Causes
Plantar fasciitis is caused by drastic or sudden increases in mileage, poor foot structure, and inappropriate running shoes, which can overload the plantar fascia, the connective tissue that runs from the heel to the base of the toes. The plantar fascia may look like a series of fat rubber bands, but it's made of collagen, a rigid protein that's not very stretchy. The stress of overuse, overpronation, or overused shoes can rip tiny tears in it, causing pain and inflammation, a.k.a. plantar fasciitis.
Symptoms
Plantar fasciosis is characterized by pain at the bottom of the heel with weight bearing, particularly when first arising in the morning; pain usually abates within 5 to 10 min, only to return later in the day. It is often worse when pushing off of the heel (the propulsive phase of gait) and after periods of rest. Acute, severe heel pain, especially with mild local puffiness, may indicate an acute fascial tear. Some patients describe burning or sticking pain along the plantar medial border of the foot when walking.
Diagnosis
A physical exam performed in the office along with the diagnostic studies as an x-ray. An MRI may also be required to rule out a stress fracture, or a tear of the plantar fascia. These are conditions that do not normally respond to common plantar fasciitis treatment.
Non Surgical Treatment
Careful attention to footwear is critical. Every effort should be made to wear comfortable shoes with proper arch support, fostering proper foot posture. Should arch supports prove insufficient, an orthotic shoe should be considered. Fortunately, most cases of plantar fasciitis respond well to non-operative treatment. Recovery times however vary enormously from one athlete to another, depending on age, overall health and physical condition as well as severity of injury. A broad period between 6 weeks and 6 months is usually sufficient for proper healing. Additionally, the mode of treatment must be flexible depending on the details of a particular athlete’s injury. Methods that prove successful in one patient, may not improve the injury in another. Early treatment typically includes the use of anti-inflammatory medication, icing, stretching activities, and heel inserts and splints. Cortisone injections may be necessary to achieve satisfactory healing and retard inflammation. In later stages of the rehabilitation process, typically after the first week, ice should be discontinued and replaced with heat and massage.

Surgical Treatment
In unusual cases, surgical intervention is necessary for relief of pain. These should only be employed after non-surgical efforts have been used without relief. Generally, such surgical procedures may be completed on an outpatient basis in less than one hour, using local anesthesia or minimal sedation administrated by a trained anesthesiologist. In such cases, the surgeon may remove or release the injured and inflamed fascia, after a small incision is made in the heel. A surgical procedure may also be undertaken to remove bone spurs, sometimes as part of the same surgery addressing the damaged tissue. A cast may be used to immobilize the foot following surgery and crutches provided in order to allow greater mobility while keeping weight off the recovering foot during healing. After removal of the cast, several weeks of physical therapy can be used to speed recovery, reduce swelling and restore flexibility.
Prevention
You can help to prevent plantar fasciitis by maintaining a healthy weight, by warming up before participating in sports and by wearing shoes that support the arch and cushion the heel. In people who are prone to episodes of plantar fasciitis, exercises that stretch the heel cord (known as the Achilles tendon) and the plantar fascia may help to prevent plantar fasciitis from returning. Ice massage also can be used on the bottom of the foot after stressful athletic activities. It is possible that strict control of blood sugar will prevent plantar fasciitis in people with diabetes, although this has not been proven.
What Is Heel Pain

Overview
Plantar fasciitis often occurs in middle-age. It also occurs in people who spend long hours standing on their feet at work, like athletes or soldiers. It can happen in one foot or both feet. It is common in sports like long distance running, dancing etc. Athletes who overpronate (rolling in or flattening feet) are especially at risk as the biomechanics of their feet place more stress to the band. Plantar fasciitis can take a long time to heal. Six months is the average time reported in medical research. There are some who will get cured after a few weeks and for others it will take more than a year. It can also become a chronic condition in which case some sort of treatment will always be needed to prevent the pain from coming back. As sooner as the condition is treated chances are it will not get chronic or in other words if you treat plantar fasciitis sooner you will get cured faster.
Causes
Patients with tight calf muscles will suffer with excessive pulling of the muscle group on the back of the heel. This in turn creates pulling of other structures that are attached to the heel, including the Plantar Fascia. When the pulling continues for long enough, then inflammation will develop and lead to Plantar Fasciitis. This causes Heel Pain. It is extremely common for patients who increase their level of activity to develop Plantar Fasciitis. Boot camp, running, zumba, recreational walking or other quick movement sports such as tennis or touch football are typical causes of Heel Pain. The sharp increase in exercise is too much for the foot to cope with and the stress on the Plantar Fascia causes inflammation. The Heel Pain that is caused by this inflammation is known as Plantar Fasciitis.
Symptoms
Heel pain is the most common symptom associated with plantar fasciosis. Your heel pain may be worse in the morning or after you have been sitting or standing for long periods. Pain is most common under your heel bone, but you also may experience pain in your foot arch or on the outside aspect of your foot. Other common signs and symptoms of plantar fasciosis include mild swelling and redness in your affected area, tenderness on the bottom of your heel, impaired ability to ambulate.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose plantar fasciitis. Occasionally, further investigations such as an X-ray, ultrasound or MRI may be required to assist with diagnosis and assess the severity of the condition.
Non Surgical Treatment
Many cases of plantar fasciitis can be treated with simple, conservative measures. These include ice packs, stretching exercises, anti-inflammatory medications, orthotic devices (custom molded orthotics), and physical therapy. It’s important to consult your doctor before you take any medications to treat this condition. In chronic or persistent cases, one of three techniques may be used to treat plantar fasciitis. Extracorporeal Shock Wave Treatment (ESWT). TOPAZ treatment. Platelet Rich P
lasma therapy.
Surgical Treatment
Surgery is rarely used in the treatment of plantar fasciitis. However it may be recommended when conservative treatment has been tried for several months but does not bring adequate relief of symptoms. Surgery usually involves the partial release of the plantar fascia from the heel bone. In approximately 75% of cases symptoms are fully resolved within six months. In a small percentage of cases, symptoms may take up to 12 months to fully resolve.
Stretching Exercises
Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It's usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Towel stretches. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Wall stretches. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stair stretches. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Chair stretches. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. Dynamic stretches. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day.